


There’s nothing pro-life about our country’s new restrictive abortion laws
There’s nothing pro-life about our country’s new restrictive abortion laws
In a post-Dobbs world, we’re creating OB-GYN deserts that put women’s lives at risk

In the wake of the Dobbs decision one year ago, women across the country spoke very publicly about their abortions — many for the first time. The phrase “I don’t regret my abortion” appeared on everything from buttons and signs to t-shirts and cakes. The idea was to end the stigma of abortion by showing people how common abortion is, to reveal that everyone knows someone (or multiple someones) who’ve had an abortion.
I’ve never had an elective abortion, but I’ve had five spontaneous abortions, commonly known as miscarriages. And while I’m not trying to conflate the two, I think the similarities they share should be an important part of the conversation because abortion care and miscarriage care are the same.
You’re getting this late because I’ve been so worried about getting this wrong.
I’ve struggled to write this piece for weeks because abortion is such a big topic and because my story is so complicated. You’re getting this late because I’ve been so worried about getting this wrong. But when I think about what is happening in women’s health care, I’m enraged. I feel powerless and pissed off. I’ve read a lot about abortion since the SCOTUS leak last May, but I have yet to hear anyone connect all the dots in the way I hope to here. Doing so involves getting personal. That may make some readers uncomfortable, but I don’t care. I believe in the power of stories and I value my personhood — and yours — way more than I value my privacy.
Between 2000 and 2006, I was pregnant eight times. All eight pregnancies were high-risk. Two of the three live births were emergency C-sections, all three babies were born prematurely, and all of them spent time in the NICU — one a few hours, one a few days, one a few weeks. Those were the happy stories.
Five of my eight pregnancies ended in miscarriage: three in the first trimester and two in the second, including one at 18 weeks. My body never fully miscarried on its own. Twice I had to have surgical procedures to remove the fetus from my uterus: One dilation and curettage (D&C) and one dilation and evacuation(D&E). I also took what is commonly known as the abortion pill once to miscarry at home.
In another time and another place things could have been much worse. I just never imagined that the other time and place would be 22 years later in the same developed country. Nor did I ever imagine that pregnancy would someday be more dangerous for my daughter than it was for me.
Making babies is a risky business in the United States of America. The U.S. is the only industrialized nation with a consistently rising maternal mortality rate — a rate has nearly doubled in the last 20 years. Pregnancy is even riskier if you’re Black: the maternal mortality rate for Black women is three times higher than that of white women. And today in the U.S., a woman is more likely to die from complications of pregnancy and birth than her mother was a generation ago.
The Dobbs decision is going to make things even worse.
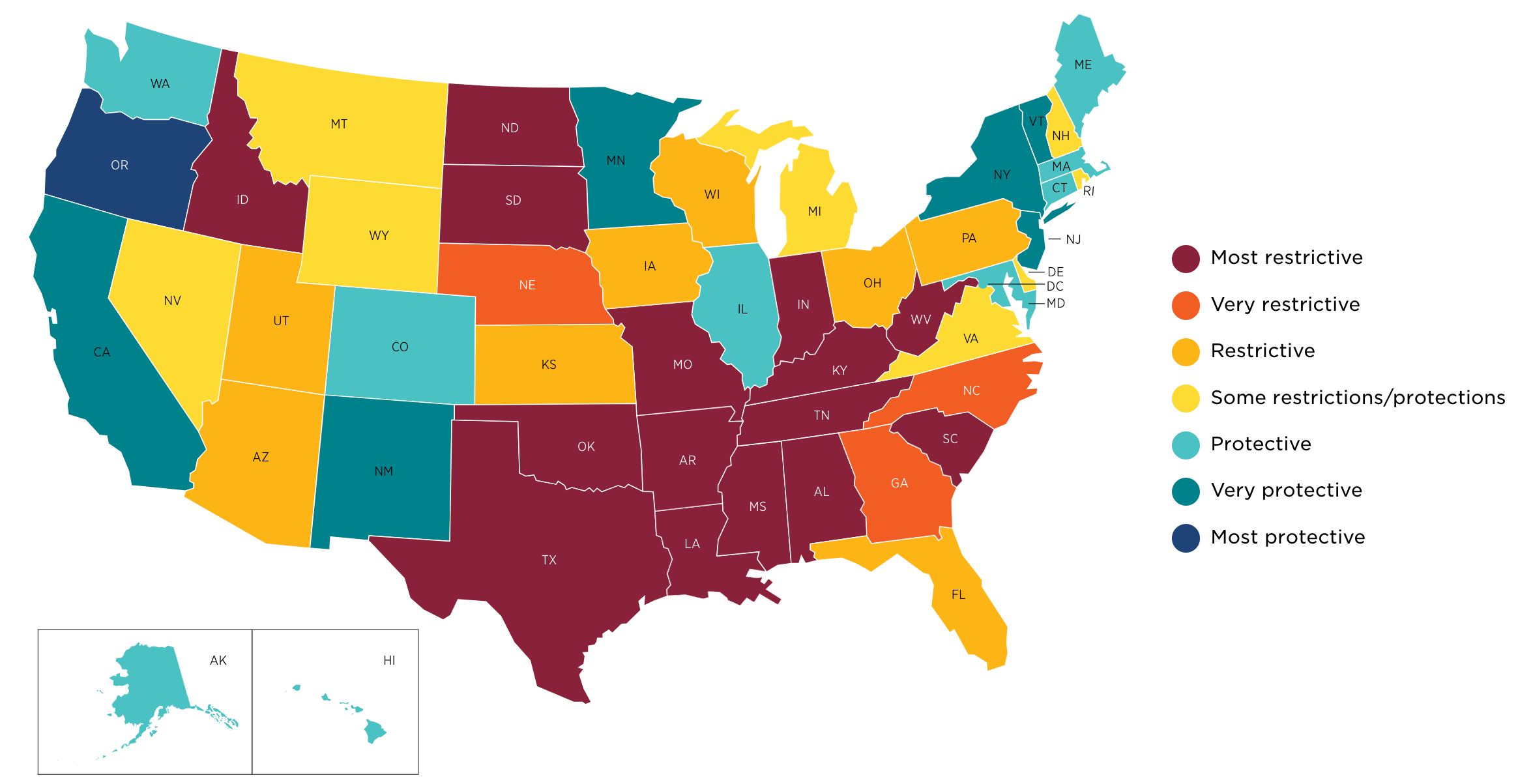
Here’s a map of the United States, showing current U.S. abortion policies and access as of October 31, 2023. Keep in mind that this map does not include “proposed bills, bills that have been signed by a governor but have not taken effect yet, or laws that are on hold because of legal challenges.”
Now, consider this. When future doctors finish medical school, they continue their education as residents, specializing in a specific field of medicine, such as obstetrics and gynecology (OB/GYN). Medical students start applying for these residencies a year before they graduate.
Charlotte Lee is a med student who made her residency choices based on this map. “I only applied to residencies where I knew I would get comprehensive abortion training,” she writes in a compelling essay for Cognoscenti. (Disclaimer for those who don’t know: I’m an editor at Cognoscenti.). “I will not practice in a place where I’m not allowed to provide the full spectrum of reproductive healthcare,” writes Lee, “and my fellow residents are making similar calculations.”
The numbers support that assertion. States that enacted abortion laws after the Dobbs decision saw a 10.5% drop in applicants for OB/GYN residencies in 2023. Emergency medicine saw a 21.4% drop.
Take a second look at that map. Doctors like Lee can do their job in blue and teal states. Maybe in yellow states. But orange and red states prohibit them from providing the full spectrum of OB/GYN care because doctors who provide abortion care do so much more than abortions.
These doctors provide miscarriage care. They treat uterine, cervical and breast cancers. They care for patients with pelvic pain, urinary tract infections (UTIs), incontinence, endometriosis, and fibroids. Oh, and let’s not forget sexual dysfunction and infertility. This map doesn’t just show where restrictive abortion policies have been enacted. It shows where women’s health care has been compromised.
Compared to states where abortion is accessible, states that have banned, plan to ban, or have otherwise restricted abortion have fewer maternity care providers, more “OB/GYN deserts,” and higher rates of maternal and infant mortality. In fact, research from the Commonwealth Fund shows that states with restrictive abortion policies had maternal and infant death rates that were 62% and 15% higher — and that’s from data that predates Dobbs. Those numbers are not going to improve — not when OB/GYNs have to do their jobs with one hand tied behind their backs.
[I]n another time and another place things could have been much worse. I just never imagined that the other time and place would be 22 years later in the same developed country.
What will women’s healthcare look like in these OB/GYN deserts in a decade or two? Imagine being diagnosed with aggressive cervical cancer in North Dakota. What if you found out your pregnancy wasn’t viable at 18 weeks in Iowa. Picture being transported to an ER in Tennessee with preeclampsia in your third trimester. Try not to think about pregnant as the result of rape in Alabama.
Yes, in theory there are exceptions. But in reality, you are screwed. Because when we outlaw abortion care, we compromise all of obstetrics and gynecology, making merely being a human with female reproductive organs riskier than it has to be. We fetishize the “unborn” at the expense of the humans capable of gestating them.
Marta Perez, an OB/GYN in Austin, TX, explains how restrictive abortion laws affect miscarriage management on Instagram (and on Twitter). For first-trimester miscarriages, Perez explains, the most effective treatment is a two-medication regime: mifepristone and misoprostol. So when laws restrict access to mifepristone based on its use for elective abortions, they’re also denying women who suffer spontaneous abortions the most effective treatment, the treatment that helps them avoid surgery.

The effect of restrictive abortion laws on second-trimester miscarriages is even more complicated — and more powerful. Sometimes at a pre-viable gestational age, the body begins to spontaneously abort the pregnancy. According to Perez, this can happen with advanced early labor, cervical insufficiency, pre-viable premature rupture of membranes (aka PROM), or abruption. In these cases, the mother risks infection and other serious complications — even death — but doctors cannot intervene while there is still a fetal heartbeat, which puts the mother’s life at risk.
“They have to wait until the person is more and more sick in order to be able to intervene,” explains Perez. “In no other part of medicine do we wait until someone is near death or very ill to intervene when preventing them from getting sick is the better option.”

Remember, says Perez, in these situations, waiting does nothing to increase the chances of viability. “All it does is make a pregnant person more sick.” This is how Savita Halappanavar, who was denied an abortion during a miscarriage died in Ireland, leading to that country’s repeal of its Eighth Amendment, which had effectively banned abortion. Halapannavar, who was miscarrying, was denied a D&E until her 17-week fetus’s heartbeat stopped, but by then it was too late. Halappanavar, a 31-year-old dentist, died of septicemia the day after the procedure.
That could have been me on more than one occasion. My due date for my first pregnancy was July 11, 2000. My water broke on May 8. At 30 weeks, the pregnancy was viable, but it was still too soon for the baby to be born. So I sat on a hospital bed for weeks, leaking amniotic fluid and hoping the baby’s lungs would develop before either it or I developed a deadly infection. My son was born at 34 weeks, but he still couldn’t breathe. That was in Alabama. I wouldn’t even visit that state if I were pregnant in 2023.
During my second pregnancy, I found out that my 18-week-old fetus no longer had a heartbeat on November 28, 2001. I don’t remember much about that day. But I do remember calling the babysitter who was at home with my 18-month-old to tell her what had happened and that we would be later than expected. I remember that she refused to let me pay her when I got home.
Even though I didn’t have to leave my own city for care, I couldn’t get a D&E for two days. I spent 48 hours pregnant, but not pregnant. I was depressed and devastated, but I had a great doctor and he had a sound plan. I cannot imagine having that miscarriage today in the yellow, orange or red states on the map above. I cannot imagine having to jump through administrative and legal hoops to prove that my D&E was “legitimate” and legal. I cannot imagine having to fight for miscarriage care in between bouts of crying in the shower because my milk had come in but there was no baby to feed.
My fourth pregnancy ended abruptly on the morning of March 24, 2003, when my uterus ruptured at home at 36 weeks. I knew this was a risk because my first C-section had been such a disaster and I tried to tell the ER staff what I suspected as soon as I arrived at the hospital. But they thought I was crazy. I wasn’t: I was right. A ruptured uterus is so rare they asked my husband to take photos of my insides for educational purposes during my C-section (apparently the operating room camera was broken). Had the uterine rupture happened earlier in the pregnancy, when my baby wasn’t viable but still had a heartbeat, in a state with restrictive abortion laws, I would have bled to death very quickly.
Despite all of this, I always loved being pregnant. I felt powerful. I felt special. Pregnancy is a miraculous thing that will never cease to amaze me. But in the U.S. in 2023, having breasts, a uterus, a cervix, ovaries and a vagina poses greater health risks than it did even a few years ago and more people need to know that.
After Ireland repealed the Eighth Amendment in the wake of Savita Halappanavar’s death, people left notes and flowers at a street-side mural that honors her. “Sorry we were too late, but we are here now,” read one message on the wall. “We didn’t forget you.”
I struggled to write this essay because the topic — and my rage — are so big. I know it’s not my greatest writing, but I also knew that it wasn’t going to get better in my head and, as recent events in Iowa underscore, we don’t have the luxury of time. In much of the United States in 2023, people like me might not survive their pregnancies and I don’t want my story to come too late. I’m here now and I hope people will listen.
Thank you so much for sharing the facts and being vulnerable in your story. My version is eerily similar and I’ve struggled with how to communicate my thoughts during the current times. In solidarity with you friend 🩵
Kate, this is so powerful. Thank you for putting it out there. I wish I could make everyone of the misogynist, ignorant legislators read it.
MTTCT
Ann